
In this article:
Bile is a greenish-yellow liquid produced by the liver that is essential for fat metabolism during digestion. It also aids in nutrient absorption, hormone metabolism, and excretion of waste materials, among other functions.

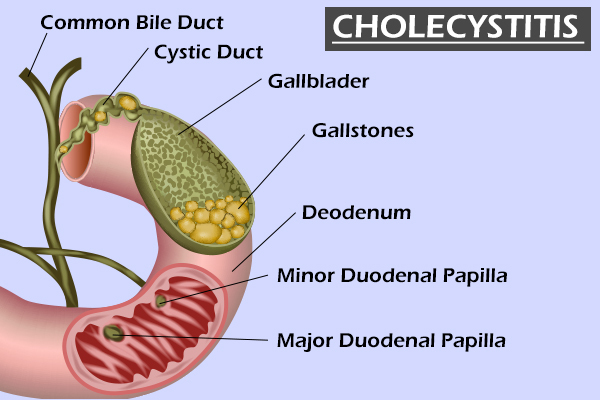
This digestive fluid flows from the liver into another small organ attached below it called the gallbladder, where it is stored. The gallbladder releases the bile into the small intestine only during the digestion process via a small duct. (1)
If this passage of bile becomes obstructed or slows down due to some reason, it starts to build up inside the gallbladder, causing inflammation. This inflammation of the gallbladder is referred to as cholecystitis. (2)
Cholecystitis can be sudden (acute) or long-term (chronic).
Types and Causes of Cholecystitis
There are two major types of cholecystitis depending upon the underlying cause:
1. Calculous cholecystitis (with gallstone formation)
Most cases of acute and chronic cholecystitis are caused by gallstones or sludge (thickened bile) that blocks the cystic duct. (3)
The cystic duct is the channel connecting the gallbladder to the common hepatic duct (one of the main bile ducts) before it empties in the duodenum (first part of the small intestine). With blockage of the cystic duct, inflammation of the gallbladder, or cholecystitis, ensues. (4)
In some cases, when the bile is infected with bacteria commonly found in the gastrointestinal tract such as E. coli, Klebsiella, Enterococcus, and Enterobacter, the inflamed gallbladder can become infected. (5)
2. Acalculous cholecystitis (without gallstone formation)
Cholecystitis can also occur without gallstones or sludge, but this is much less common. This condition is referred to as acalculous cholecystitis. It is usually caused by slowing of gallbladder emptying, leading to stagnation of bile. (4)
The most commonly affected by the occurrence of acalculous cholecystitis are the severely ill in the intensive care unit. These patients are typically not eating, leading to stasis of the gallbladder.
Because the gallbladder is not emptying normally, the concentration of bile and the pressure within the gallbladder increase. (6) The stoppage of bile flow also increases the risk of infection, which paves the way for more serious complications.
In many cases, the exact cause of acalculous cholecystitis is unknown.
Signs and Symptoms of Cholecystitis
Up to 11% of patients with gallstones develop symptoms, while the majority of patients go through life unaware of having them. Symptoms of cholecystitis can be insidious, ranging from very mild to more typically right-upper-quadrant pain.
Abdominal pain worsened by eating is typical of acute cholecystitis since gallbladder emptying is stimulated by eating a fatty meal. (7) The pain has a sudden onset and is often accompanied by fever and an elevated white blood cell count. (8)
Chronic cholecystitis is associated with mild abdominal pain or no symptoms at all.
Treatment for Cholecystitis
Cholecystitis requires hospitalization, and treatment begins with supportive measures such as intravenous fluids, pain control, and antibiotics. (9) Patients are not allowed to eat to avoid stimulating the gallbladder.
Surgical removal of the gallbladder is the definitive treatment for cholecystitis and is usually performed within 72 hours of the onset of symptoms in uncomplicated cases. (10) But this timing can vary in more complicated cases.
Diagnosing Cholecystitis

The diagnosis is made first by abdominal ultrasound showing thickening of the gallbladder wall and fluid around the gallbladder and a sonographic Murphy’s sign (tenderness in the right upper quadrant of the abdomen elicited by the ultrasound probe). (11)
The HIDA scan (hepatobiliary iminodiacetic acid scan) or cholescintigraphy can be helpful in confirming the diagnosis. (12) The gallbladder is not visualized with cholecystitis on a HIDA scan due to blockage of the cystic duct.
Magnetic resonance cholangiopancreatography is utilized if blockage of the common bile duct is suspected in cases of acute cholecystitis. (13)
Risk Factors for Cholecystitis
The risk factors for gallstone formation include:
- Female gender
- Pregnancy
- Hormone therapy
- Old age
- Native American race
- Hispanic ethnicities
- Obesity
- Rapid weight loss
- Cirrhosis of the liver
- Diabetes
Complications Associated With Cholecystitis
Complications of acute cholecystitis include a gangrenous gallbladder, perforation, emphysematous cholecystitis, cholecystoenteric fistula, and gallstone ileus.
- A gangrenous gallbladder means that the gallbladder tissue begins to die as it fails to receive proper blood flow. This occurs in 20% of cases of acute cholecystitis and is characterized by severe infection of the gallbladder and usually with systemic infection as well. (14)
- The dead tissue of the gangrenous gallbladder can tear easily and develop a hole. This perforation opens a connection between the gallbladder and the intestine, which is known as cholecystoenteric fistula.
- If a large gallstone >2.5 cm in diameter passes through the fistula, it can cause blockage of the small intestine, which is known as gallstone ileus. (15)
- When the gallbladder becomes infected with gas-forming bacteria such as Clostridium welchii, air forms in the wall of the gallbladder, leading to emphysematous cholecystitis.
When to See a Doctor

A doctor should be consulted with the onset of unexplained abdominal pain that is:
- Recurrent
- Severe
- Persistent for more than a few hours
- Accompanied by other symptoms, such as jaundice and a fever
Final Word
Pay heed to the warning signs of cholecystitis and seek immediate medical help. This condition is characterized by abdominal pain that may be sharp and sudden in acute cases or mild and recurrent in chronic ones.
Whatever the case, you must seek immediate medical consultation because delayed treatment can result in serious complications.
- Was this article helpful?
- YES, THANKS!NOT REALLY